What is Social Banking?
Social Banking enables customers of banks to conduct their banking activities through social media sites such as Facebook, Twitter, etc. Social Banking is a new initiative started by banks to cater to the current online behaviors of today’s young generation who spend a big chunk of their daily time on social media sites especially on their mobile phones.
Considering that banking is a industry where change is slow, social banking is a new bold attempt to attract the young generation. But is this new initiative really catching on with the young generation?
We will look at few examples of Social Banking in India, the current mindset of customers towards Social Banking and barriers, and few steps to design a social banking experience.
Examples of Social Banking in India
- Download a bank’s mobile app to create an account by taking a selfie and enter few relevant details including the customer’s national identity information to create a bank account in few minutes.
- Pay utility bills through Facebook Messenger.
- Meet bank employees virtually through video branch services.
- Follow a bank’s Twitter account to pay a friend.
- Interact with a robot at the bank branch regarding information on banking transactions.
- UPDATE: Example of a mailer inviting credit card applications with the promise of efficient and quick interaction through a chatbot (mailer received on July 15, 2017).

Current mindset of customers towards Social Banking
Ideally, this new initiative is targeted towards the audience segment who spend a great time on social media platforms. However, what is worrying that the youngsters see social banking as a cool feature rather than a transactional channel like the bank’s mobile app or website.
Main barriers against adoption of Social Banking
Comfort and convenience with existing digital channels
Today’s young generation are comfortable accessing their own bank’s mobile or website or with third-party payment apps such as Paytm or Phonepe. The above digital channels are easy to use and their user experience is high thus retaining these existing customers.
Perceived view of social media platforms
Customers see social media platform as a place to share information at their pace surrounded by friends whereas banking is perceived to be a private and secure activity conducted in a safe and secure environment. A banking activity is thought to be important whereas activities on social media platforms are seen as fun and not important.
Lack of awareness with existing customers
Banks market social banking as a new cool feature but its recall value is very limited. Two of my friends, who are regular users of Facebook were not sure whether their bank offered such services even though their banks did advertise on their website, which included an interactive demo.
Steps to design a Social Banking experience
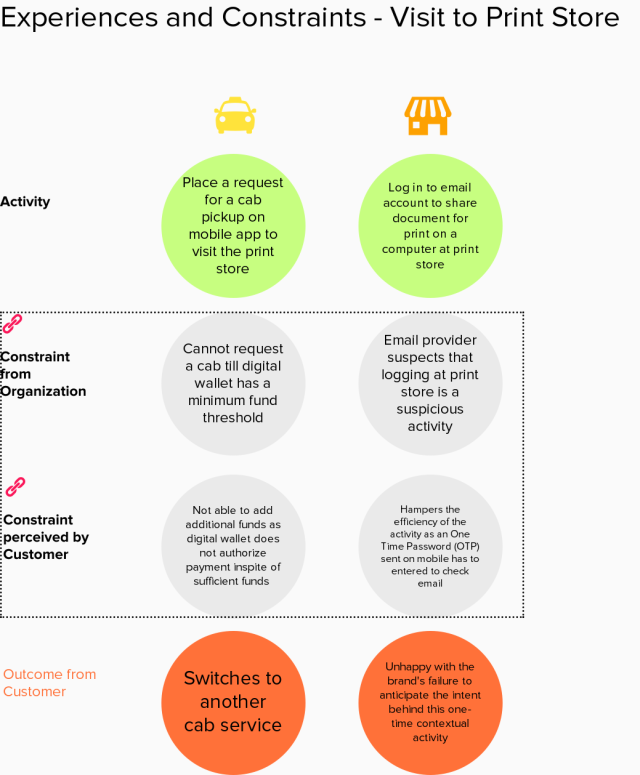
Banks see social banking as a new way to engage with the younger generation in addition to their transactional activities with the existing touchpoints. Banks might not have full control over their social banking experiences as it is dependent on the specific social media’s platform’s user experience. So, customer experience is partially impacted by the specific social media’s platform and the integration of the bank’s service with the social media platform. Hence, there is a high possibility that the customer experience of social banking will be definitely fragmented.
Sharing steps below to design a better social banking experience:
- Zoom out to learn about the customer’s daily life activities rather than focusing on the specific banking customer journey.
- Learn about the customer’s social media behaviors.
- Learn about the customer’s current usage of bank’s touchpoints.
- Implement gamification and behavior change techniques to help customers to be at ease when conducting banking activities with their preferred social media platforms.
- Monitor the usage on the social media platforms and prototype as necessary with new ideas till the customers find it easy to switch between their current touchpoints and preferred social media platforms to conduct banking activities.
Time to shift to an engaging conversation
Current usage of digital touchpoints enable the banks to save time and resources but risk seeing the customer as a disparate set of data points rather than engaging them at a human level to know about their financial needs in their life. With the introduction of social banking, banks have a good opportunity to shift the transactional nature of digital interactions into more meaningful conversations with their customers.